
The Materials Characterization Facility (MCF) at Georgia Tech has installed a new inorganic m spectrometry facility. The facility includes two new inductively couple plasma mass spectrometry (ICP-MS) systems: a Thermo iCAP RQ quadrupole ICP-MS for streamlined and high-throughput determinations of elemental concentrations and a Thermo Neoma multicollector ICP-MS with collision cell technology for the precise determinations of isotope ratios within a given sample.
Each instrument can measure elemental variability in both dissolved aqueous samples as well as solids/minerals via laser ablation microsampling from a Teledyne Iridia laser ablation system. Together the system can measure isotopes at precision in elemental systems from Li and U.
Planned applications include: (1) high-resolution measurements of Ca, Sr, Ba, Mg, and B elemental and isotopic variability in seawater and marine and terrestrial carbonates for paleoclimate reconstructions, (2) (U-Th)/Pb dating and Hf isotope measurements to study the origin of critical mineral deposits, with a potential engineering application and the development of novel methods for increasing precision/accuracy and minimizing sample consumption during routine analyses of water quality and environmental contamination.
The MCF welcomes users interested in these and other potential applications of this new facility to their scientific and engineering research to contact David Tavakoli (atavakoli6@gatech.edu).
News Contact
David Tavakoli (atavakoli6@gatech.edu).



When one or more coronavirus vaccines receives FDA emergency use authorization, it will launch a public health and logistics initiative unlike any in U.S. history.
Hundreds of millions of doses will have to distributed nationwide and kept cold until healthcare professionals can administer not one, but two doses to each person. And enough skeptical members of the population will have to be persuaded to receive the vaccine to slow virus transmission.
Beyond those challenges, the distribution effort will have to adapt to unexpected and uneven demand; accommodate recipients who may not return on time for a second dose; train hundreds of thousands of staff from clinics, pharmacies, doctor’s offices, and hospitals; prioritize serving high-risk groups first while encouraging others to wait — all while under tremendous pressure to get the much-anticipated vaccines into use as case counts and the death toll continue rising.
“Time is of the essence because the virus is already so widespread,” said Pinar Keskinocak, the William W. George Chair and professor in the H. Milton Stewart School of Industrial and Systems Engineering (ISyE) and director of the Center for Health and Humanitarian Systems at the Georgia Institute of Technology. “With the pressure on our timeline, knowledge of how quickly the disease is spreading, and the broad U.S. and global need, I can’t think of a comparable public health initiative that has ever been undertaken.”
Shipping and Keeping Hundreds of Millions of Doses Cold
Three vaccines, produced by Moderna, Pfizer and its German partner BioNTech, and Oxford-AstraZeneca, are expected to be available first. The Pfizer-BioNTech vaccine will need to be kept ultra-cold — minus 94 degrees Fahrenheit — on its journey to individual Americans. The Moderna drug won’t have such demanding conditions, but both it and the Pfizer vaccine will tax the existing “cold chain” that keeps vaccines and other temperature-sensitive products in a narrow range of conditions during transport and storage.
The Oxford-AstraZeneca vaccine will have much less stringent requirements and faster ramp-up in capacity, though early testing suggests its efficacy may be lower than the others. That will create tradeoffs between efficacy versus access and speed in distribution.
Plans already exist to get the vaccines from manufacturers to the states, each of which has developed its own distribution plan. Keskinocak worries mostly about “last mile” plans — getting the vaccines to where they will be injected — and getting individuals to those locations.
“Access is going to be a challenge,” she said. “You may be able to get it to locations where it can be distributed, but you have to make sure the people who really need the vaccine can easily access those locations.”
Cold chain transportation, tracking, tracing, and storage already exist in most areas, but refrigeration could be challenging for rural areas that may be at the end of the chain, especially for the vaccine requiring very cold temperatures beyond the capability of freezers found in most doctor’s offices and clinics. And cold can sometimes be too cold, Keskinocak said.
“We often think about keeping it cold, but sometimes it may be too cold, which is not good. It’s not just whether the temperature exceeded the required level, but also whether it went below that. It is important to keep the vaccine exactly at the required temperature level.”
Pfizer has developed a shipping container that includes a temperature tracking device — and 50 pounds of dry ice to maintain the right temperature during transit. Because it is contained in small vials and the liquid vaccine is diluted for use, the overall volume being shipped will be relatively small, limiting the number of packages that will be moved and stored, Keskinocak noted.
Ultimately, the cold chain may play a significant role in vaccine effectiveness. Currently, the vaccines being produced by Pfizer/BioNTech and Moderna are reported to have a higher efficacy than the Oxford-AstraZeneca vaccine — but only if they can be maintained at the proper temperatures. The timing, magnitude, and duration of temperature fluctuations during transport and before administration could affect that in ways that may be difficult to assess.
“Our current modeling shows that a vaccine that is less effective but that can be distributed more quickly and more widely might work better in some settings than a more effective vaccine, thereby reducing the total number of infections in the population,” Keskinocak said.
If You Build It, Will They Come?
Expectations are that the nation is hungry for a vaccine to escape the horrors of Covid-19. But a recent Gallup survey shows that only 58% of respondents said they planned to receive the vaccine when it becomes available. Boosting that percentage will require a massive communications effort to overcome vaccine reluctance and concerns fueled by the uneven nature of the U.S. pandemic response.
“If we can get the vaccine to locations where people can access it, and we have the necessary syringes, supplies, and PPE, as well as the healthcare staff to administer the injections, it’s not clear that people will come to receive it in large enough numbers,” Keskinocak said. “That’s one major component missing from a lot of the plans that I see at the state level.”
The communications program will have to run in parallel to the vaccine distribution, and they have to be coordinated so that supply meets demand.
“Public health communication and dissemination of information at the right time and in the right language is going to be at least as important and challenging as the logistics of distributing the vaccine,” Keskinocak said. “Communication is going to shape demand to a large extent. If one is more effective than the other, we will have a mismatch between demand and supply.”
Different demographic populations have different levels of trust for medicine in general and vaccines in particular, she said, so communications campaigns will have to focus on issues of concern to those groups. Unexpected variations in vaccine demand caused by these concerns could also create logistical uncertainties.
“We can try to forecast demand, and ship supplies to those locations,” she said. “But historically, we have seen that demand can exceed supply in one location while inventory builds up in another location. We need to avoid this situation of unmet demand and unused vaccine.”
Another issue will be the two doses necessary for the vaccine. The second dose must be received within a narrow range of time for the two-dose vaccine to be effective. Should a second dose be reserved for every person receiving a first dose, or should the goal be to get as many doses out as possible?
“Some people may never show up to be vaccinated, while others will receive the first dose, but may not come back for the second dose,” she said.
Getting the Program Started
The first available doses will likely go to healthcare workers and first responders who are on the front lines of battling Covid-19. That is expected to be the easier part of vaccination logistics, and the lessons learned there should help with the much more massive vaccination campaign for high-risk individuals and the general public.
As vaccine production and distribution capacity ramp up, other groups will be next in line. While distributing small batches as manufacturers produce it can create some supply challenges, that also allows the system to more easily adjust to unexpected demand.
Even though distributing and administering vaccines is something the U.S. healthcare system does routinely, the size and timeline of this project are unprecedented, Keskinocak noted.
Beyond the logistical and communications needs, the vaccination program will also have a strong information technology component. Administration will likely be by appointment, and each injection will have to be reported to a vaccine registry to provide a record of which vaccines people have received and when.
Vaccinating People Who May Already Be Immune
It’s estimated that the number of reported Covid-19 cases may be just 10% of the actual number of infections in the U.S. Assuming recovery from the virus confers immunity for some period of time means there may be quite a few people who don’t actually need the vaccine right away to be protected. But there are currently no plans to determine whether recipients are already immune before they receive the vaccine.
“There are a lot of people out there who have some level of immunity to the coronavirus,” Keskinocak said. “The plans I’ve seen don’t include the serological testing that would be needed to identify people with some level of immunity, which could be around 30% of the population by the time the vaccine gets out to the general public.”
Testing for immune antibodies could be done ahead of the vaccination program, but that would create an extra step in a process that is already quite complicated. Healthcare systems such as the U.S. Department of Veterans Affairs or certain private insurance plans could include that step, especially if vaccine supplies lag behind demand.
“The big complexity is timing,” she said. “Once vaccines become available, you’ll want to deliver them as quickly as possible to as many people as possible in a very short time frame.”
Annual vaccination campaigns for the seasonal flu set ambitious goals for the population levels they want to reach, but the time challenges will be much greater for the coronavirus vaccine.
“The seasonal flu vaccine becomes available months before the virus spreads broadly, so we have quite a bit of time to administer it before we get into the peak of the flu season,” she said. “We have been in the midst of the Covid-19 pandemic for several months now. We are really late in the game, so we don’t have the luxury of time.”
Keskinocak is cautiously optimistic that the challenges will ultimately be addressed.
“There are certainly still lots of unknowns,” she said. “But the state plans I have seen look reasonable from a supply chain standpoint. Some of the decisions will be made once the states receive the vaccine, and exactly how they do it will be somewhat up to the local jurisdictions. There are still many things that need to be decided to make this unprecedented initiative live up to its goals.”
Research News
Georgia Institute of Technology
177 North Avenue
Atlanta, Georgia 30332-0181 USA
Media Relations Contact: John Toon (404-894-6986) (jtoon@gatech.edu)
Writer: John Toon
News Contact
John Toon
Research News
(404-894-6986)

BioFabUSA, a Department of Defense-funded Manufacturing Innovation Institute within the Manufacturing USA network, has awarded the Georgia Institute of Technology and industry partner, Akron Biotech, a project titled, “Supply Chain and Process Modeling Algorithms, Methods, and Tools for Tissue Manufacturing and Distribution”. This project will address significant national supply chain issues related to distributing tissue engineered medical products (TEMPs) to U.S. patients in need.
The project aims to create the first simulation-based supply chain model for the rapidly evolving and future facing TEMPs industry, to minimize manufacturing and logistics costs and risks, incorporate Department of Defense (DOD) and other stakeholders’ perspectives into supply chain modeling, inform standards development, and support workforce development.
“Having a supply chain model will be instrumental in helping new and existing companies plan for the most efficient process flows, resource usage, and cost savings,” said Stephanie Robichaud, technical project manager with the Advanced Regenerative Manufacturing Institute. “Many startup companies do not realize some of the intricacies in managing their supply chain and many established companies realize the importance of it after experiencing inefficiencies. Having a model that these companies can use will help advance the field of tissue engineering as they plan for scale-up.”
According to Ben Wang, executive director of the Georgia Tech Manufacturing Institute (GTMI) and professor in the Stewart School of Industrial and Systems Engineering, “hundreds if not thousands of patients are waiting for tissues and organs in order to have a normal healthy life. Our project is a bold initiative to democratize distribution of replacement tissues and organs by streamlining national supply chains. This project will develop simulation-based tools to enhance the efficiency and resilience of the TEMPs supply chain, making these personalized medicines more affordable and more accessible.”
The growth of the TEMP industry is going to change the supply chain of medical tissues disruptively. To embrace this change, a system-level decision support tool is essential for adopting more cost-effective manufacturing processes and making better investment decisions. To ensure successful commercialization and adoption of this new supply chain decision support tool, the project team will engage multiple stakeholders including DOD, government, regulatory bodies, standards setting organizations, patients, industry, academia, policy experts, education and workforce development experts.
Georgia Tech project leads include Ben Wang, Ph.D., Chelsea C. White III, Ph.D, and Kan Wang, Ph.D. Ben Wang is Gwaltney Chair in Manufacturing Systems, professor in the Stewart School of Industrial & Systems Engineering and School of Materials Science and Engineering at Georgia Tech. In addition, he serves as executive director of the Georgia Tech Manufacturing Institute (GTMI). Chelsea C. White III is the Schneider National Chair in Transportation and Logistics and professor in the H. Milton Stewart School of Industrial and Systems Engineering at Georgia Tech. Kan Wang is lead researcher of additive manufacturing in the Bio-Engineering Research Laboratory at GTMI.
Leading the project for Akron Biotech is Ezequiel Zylberberg, Ph.D, who is vice president of product development and planning. According to Ezequiel, “the future of regenerative medicine depends on more than our ability to address the scientific challenges of generating the next generation of advanced therapies. Advancing these novel treatments in a way that is scalable will require significant advances in manufacturing innovation. We are eager to collaborate with our colleagues at Georgia Tech, at BioFab USA, and throughout the regenerative medicine industry to confront the challenge of scalability and supply chain resilience through this modelling effort.”
About the Georgia Institute of Technology
The Georgia Institute of Technology, also known as Georgia Tech, is one of the nation’s leading research universities — a university that embraces change while continually Creating the Next. The next generation of leaders. The next breakthrough startup company. The next lifesaving medical treatment.
Georgia Tech provides a focused, technologically based education to more than 36,000 undergraduate and graduate students. The Institute has many nationally recognized programs, all top-ranked by peers and publications alike, and is ranked among the nation’s top five public universities by U.S. News & World Report. It offers degrees through the Colleges of Computing, Design, Engineering, Sciences, the Scheller College of Business, and the Ivan Allen College of Liberal Arts. As a leading technological university, Georgia Tech has more than 100 centers focused on interdisciplinary research that consistently contribute vital research and innovation to American government, industry, and business. https://www.gatech.edu/
About Akron Biotech
Akron is a leading materials manufacturer and services provider to the regenerative medicine industry, accelerating the development and commercialization of advanced therapies. Founded in 2006, Akron is an ISO 13485-certified company that operates in line with cGMPs and international standards, enabling advanced therapy developers to de-risk their supply chains and facilitate regulatory approval. The company's unique business model emphasizes knowledge, flexibility and unparalleled service—from development through to commercialization. For more information, please visit www.akronbiotech.com.
About BioFabUSA
BioFabUSA, is a DOD-funded Manufacturing USA Innovation Institute (MII) sustained by the Advanced Regenerative Manufacturing Institute (ARMI) is a non-profit organization located in Manchester, New Hampshire. ARMI's mission is to make practical the scalable, consistent, cost-effective manufacturing of tissue engineered medical products and tissue-related technologies, to benefit existing industries and grow new ones. https://www.armiusa.org/
Georgia Tech Manufacturing Institute
813 Ferst Drive, NW
Atlanta, GA 30332 USA
Media Relations Contact: Walter Rich (walter.rich@research.gatech.edu)
News Contact


Personal initiatives by a pediatrician and by researchers to make face shields for medical workers have transformed into an industry collaboration that by June had delivered 1.8 million shields to hospitals and other organizations around the country with plans to produce 2.5 million all total. A $2 million donation from Aflac Incorporated for personal protective equipment (PPE) financed the bulk of the shields.
To make it happen, a team of researchers and industry partners convened at the Global Center for Medical Innovation (GCMI), a Georgia Tech-affiliated nonprofit that guides new experimental medical solutions to market. The group combined the physician’s vision with the researchers’ original designs, adjusted them to pass FDA emergency guidelines, and then coordinated mass production and distribution.
A physician’s wisdom
The project grew wings in mid-March, after Dr. Joanna Newton became concerned that the nationwide shortage of PPE was leaving healthcare workers across the country vulnerable. Newton is a physician specializing in improving healthcare safety through technology at Children’s Healthcare of Atlanta, and she was already collaborating with Georgia Tech on other projects.
She grabbed the phone to leverage the connection.
“I called Sherry Farrugia to tell her about my idea to 3D-print PPE. We needed to quickly find a solution for the PPE shortage around the country, and I knew we had the right team here in Atlanta to help,” said Newton, a pediatric hematologist/oncologist at the Aflac Cancer and Blood Disorders Center of Children’s.
“The situation was urgent, and I knew who would have the right expertise to get this done,” said Farrugia, chief operating officer and strategy officer of Children’s Healthcare of Atlanta Pediatric Technology Center, which is part of Georgia Tech.
Farrugia had Newton present her idea at GCMI to researchers, advisors, and industry partners who immediately put together a team to address the need for face shields to protect healthcare workers from droplets containing the coronavirus. She also discussed the need with Devesh Ranjan, associate chair of the George W. Woodruff School of Mechanical Engineering, who suggested connecting the effort to a parallel initiative in that school.
Bringing in engineers
At the same time, along with Ranjan, Sam Graham, chair of the George W. Woodruff School of Mechanical Engineering, and Susan Margulies, chair of the Wallace H. Coulter Department of Biomedical Engineering, were coordinating efforts across campus to develop various medical devices in response to the pandemic. Graham, Margulies, and Ranjan quickly connected GCMI with Christopher Saldana and Saad Bhamla, faculty members in Georgia Tech’s College of Engineering, who were leading an simultaneous effort to address the face shield problem with their students using rapid fabrication techniques like 3-D printing, laser cutting, and waterjet cutting.
“The Georgia Tech mechanical engineering team used rapid fabrication equipment and quickly produced multiple face shield designs that could be manufactured in high volumes for the rapid response environment that Covid-19 required,” Saldana said.
Making a few thousand shields in a lab had likely already saved lives, but the Georgia Tech researchers and GCMI put their designs on the internet, where they have been downloaded thousands of times by organizations manufacturing them around the world. And the manufacturing partners they engaged have been turning out hundreds of thousands of shields to save many more lives.
“You may need 45 minutes for a headband with a 3D printer, but manufacturers turn out six of them every 19 seconds. Then making a million face shields becomes a real possibility,” said Mike Fisher, who leads product development at GCMI.
GCMI opened a GoFundMe page, which brought in $20,000, and then engaged their first manufacturing partner, Delta Air Lines.
A manufacturing explosion
“Delta converted one of their groups from manufacturing airplane interiors to doing the face shields. They started off by manufacturing 6,000 shields, and that got the momentum going,” Leiter said. “Two thousand shields went to Mount Sinai Hospital in New York; 2,000 went to Piedmont Healthcare in Atlanta; and 2,000 went to Children’s Healthcare of Atlanta.”
Things began to snowball.
Graham engaged Siemens Industries to fulfill a face shield order from the Georgia Emergency Management Agency (GEMA) for distribution in Georgia. Partners from ExxonMobil began looking for more potential manufacturers. And Aflac contacted Children’s looking for worthy Covid-19 related efforts to support.
“We asked for a donation of $500,000 for manufacturers to retool their operations. Aflac made a gift of $2 million to GCMI to promote the production of PPE,” Farrugia said. “We were able to buy tooling for an automotive plastics manufacturer called Quality Model in South Carolina, and they have made over 750,000 face shields so far.”
GCMI won a bid from the Federal Emergency Management Agency (FEMA) for 1,141,600 face shields, which are being made by Quality Model, where ExxonMobil helped rearrange production lines for shields.
Siemens made an additional 100,000 shields from Aflac’s gift, which is also being used to purchase existing PPE to donate to healthcare workers. Kia Motors quickly produced an initial 15,000 shields, which the company financed itself.
“Kia got the open source design from the Georgia Tech website and ran with it on their own,” Saldana said.
These partners are delivering the following number of shields: Quality Model, 1,251,600; Kia Motors, 300,000; Siemens Industries, 205,000; Delta Air Lines, 106,100; Georgia Tech, 20,000; and EIS, 15,000. And more are still to come.
The shields went across the country, from hospitals in New York City to Prisma Health in South Carolina, to nursing homes in the Pensacola area, and to rural Louisiana and Mississippi, Leiter said.
Thanks in large part to Aflac’s gift, GCMI and Farrugia are coordinating with partners, including Georgia Tech engineers, to produce N95 masks, hospital gowns, and hand sanitizer, all redesigned for the Covid-19 age.
Research News
Georgia Institute of Technology
177 North Avenue
Atlanta, Georgia 30332-0181 USA
Media Relations Assistance: John Toon (404-894-6986) (jtoon@gatech.edu).
Writer: Ben Brumfield
News Contact
John Toon
Research News
(404) 894-6986

Gaps in the supply of coronavirus tests are propelling initiatives to fill them across the country. At the Georgia Institute of Technology, bioscience researchers are burning the midnight oil to produce key components for tests in the state of Georgia.
The goal is to supply a broad initiative by the governor’s office involving multiple universities and partners to rapidly produce and administer more tests. At least 35 volunteers at Georgia Tech, while adhering to social distancing, are reorienting labs normally used for scientific discovery to do larger-scale production of biochemical components.
“We are inventing new ways of doing things like an electronic buddy system so people can be alone – but not alone – while they work in the lab. The technical part is actually the easiest. The logistics of testing, data security, and regulatory considerations – those things are more challenging,” said Loren Williams, a professor in Georgia Tech’s School of Chemistry and Biochemistry.
Williams and the researchers are supporting Georgia Governor Brian Kemp’s COVID-19 State Lab Surge Capacity Task Force, which is a project managed through the Georgia Tech Research Institute (GTRI). GTRI is also leading the coordination and integration of data management across the lab surge effort.
“We are providing technical and project management of the effort which is focused on increasing the state’s ability to expand testing beyond current limitations,” said Mike Shannon, GTRI’s lead in the project and a principal research engineer at GTRI.
Exoplanets and coronavirus
The science behind coronavirus testing is complementary to the researchers’ usual work. That includes understanding proteins associated with glaucoma, figuring out how RNA and DNA evolved in the first place, or whether ribosomes – lumps of RNA and protein key to translating genetic code into life – may exist on exoplanets.
Williams’ research team studies the last topic, and some of their work is related to the core of coronavirus testing, a chemical reaction that amplifies the virus’ genetic fingerprint. It is called a reverse transcription polymerase chain reaction (RT-PCR), and it transcribes trace amounts of coronavirus’ RNA code into ample amounts of corresponding DNA in the lab for easy analysis.
“His lab members are very familiar with RT-PCR, and when the lack of tests became apparent, they swung into action. The group grew from there, based on the technical needs for the project,” said Raquel Lieberman, another leading scientist in the effort and also a professor in Georgia Tech’s School of Chemistry and Biochemistry.
“Every day, very talented, hardworking people with perfect skill sets come out of the woodwork and ask to help,” Williams said.
The group has teams that engineer the production of enzymes or other chemicals needed for RT-PCR to work: Two central enzymes are reverse transcriptase, which converts RNA to DNA and Taq polymerase, which rapidly replicates DNA. Another important component is ribonuclease inhibitor, which slows coronavirus RNA decay.
Global COVID allies
Other researchers develop processes for mass production or implementation of COVID-19 safety procedures; the list goes on. Some colleagues telework; others work in labs but spaced far from each other while they wear masks.
“The group is planning to produce enough enzyme components for hundreds of tests per day,” said Vinayah Agarwal, an assistant professor in Georgia Tech’s School of Chemistry and Biochemistry and School of Biological Sciences. “Using these components, we will also build cheaper and more robust testing kits going forward.”
Instructions already exist for some of the ingredients for the test, but they are not readily available because the rights to them are exclusive.
“Intellectual property and other proprietary issues hinder our effort,” Lieberman said. “But we have received help from scientists all over the world to piece together protocols on how to make what we need.”
The state wants to increase current testing capacities by 3,000 more tests per day. The task force also includes teams from Augusta University Health System, Georgia State University, Emory University, University of Georgia, and the Georgia Public Health Laboratory. The task force lead is Captain Kevin Caspary who is with the Georgia National Guard.
Raw footage and images as press handouts for journalists. (No commercial or personal use):
https://www.dropbox.com/sh/f2wc2i74lz1lffl/AADLJ8dQnZMr4uEDxAiIMusoa?dl=0
Also read this: Interactive COVID-19 tool shows the importance of staying at home
External News Coverage:
NPR - Sun Rays, Disinfectants And False Hopes: Misinformation Litters The Road To Reopening
News-Medical.Net - Georgia Tech researchers create key components for COVID-19 tests
Georgia Tech News Center- A New Normal: Researchers Across Georgia Tech Rally to Fight COVID-19
Here's how to subscribe to our free science and technology email newsletter
Writer & Media Representative: Ben Brumfield (404-272-2780), email: ben.brumfield@comm.gatech.edu
Georgia Institute of Technology
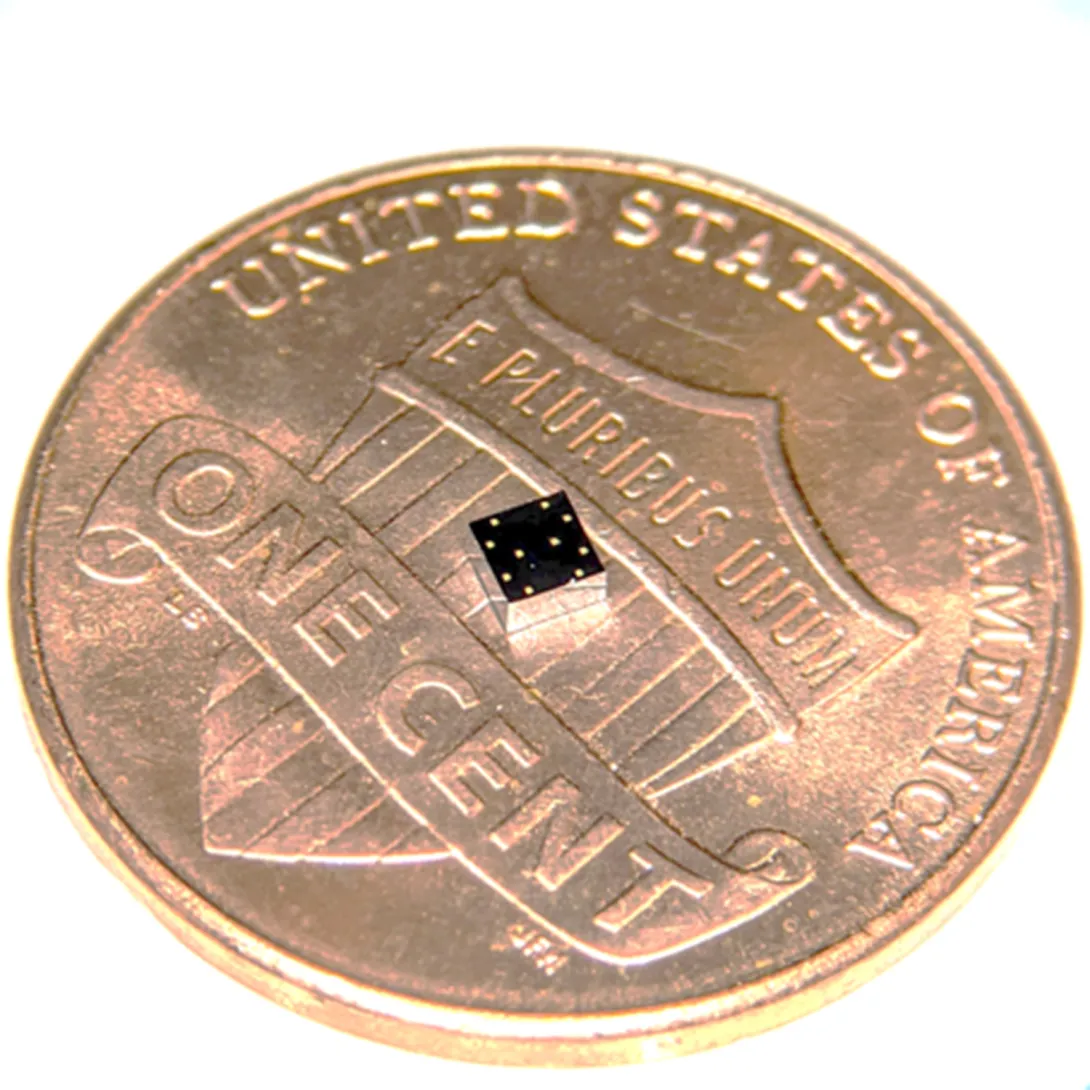
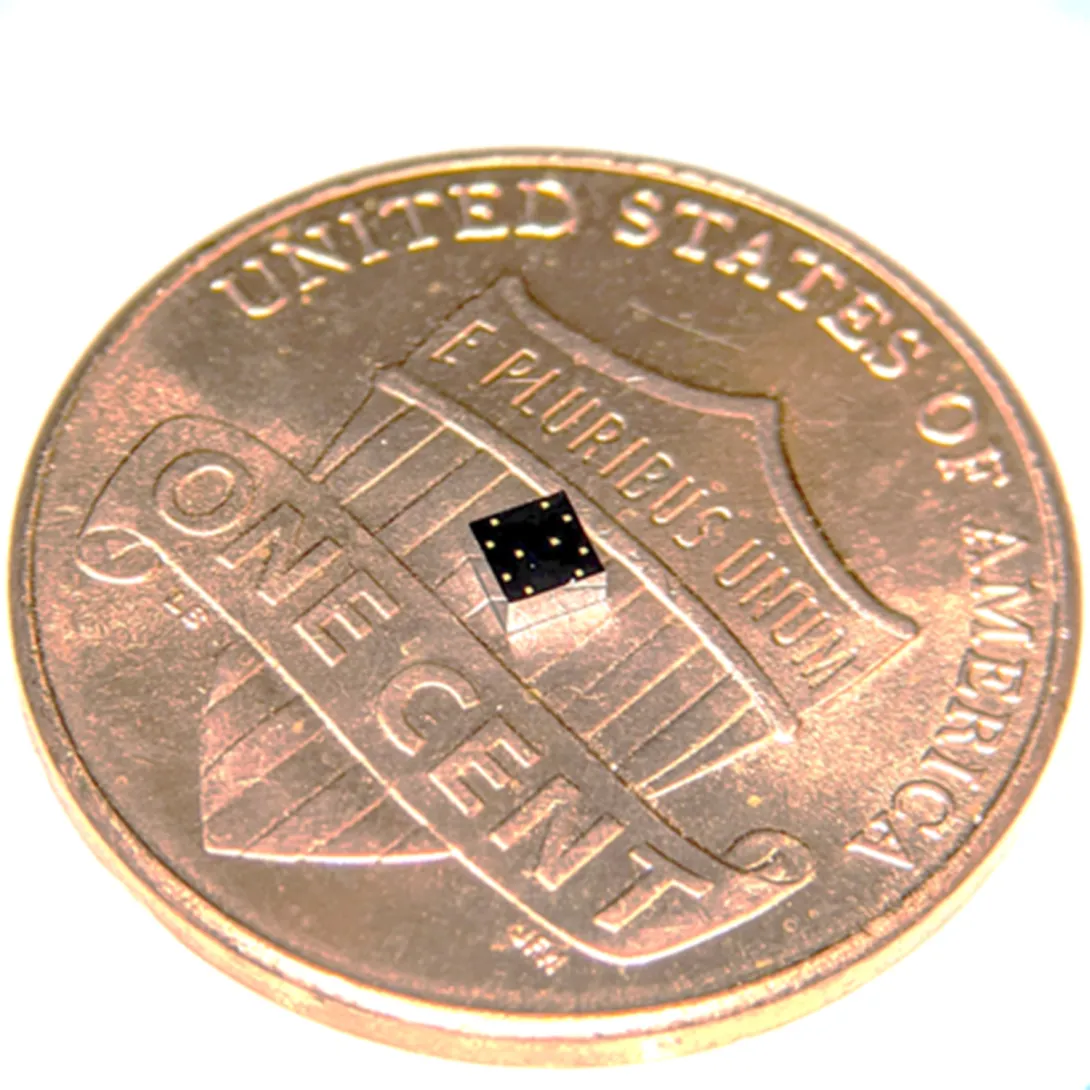
During a stroll, a woman’s breathing becomes a slight bit shallower, and a monitor in her clothing alerts her to get a telemedicine check-up. A new study details how a sensor chip smaller than a ladybug records multiple lung and heart signals along with body movements and could enable such a future socially distanced health monitor.
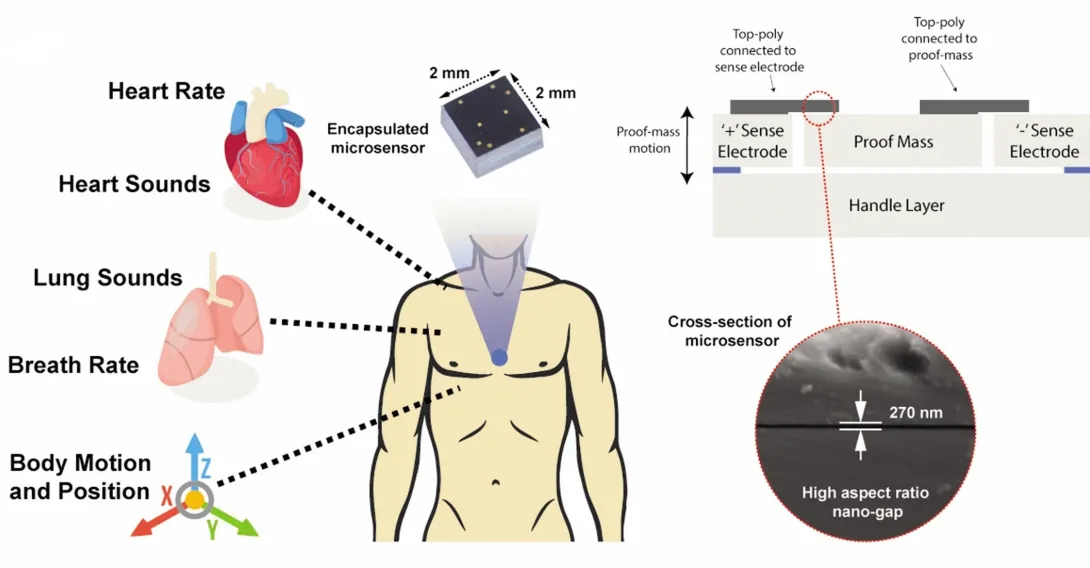
The core mechanism of the chip developed by researchers at the Georgia Institute of Technology involves two finely manufactured layers of silicon, which overlay each other separated by the space of 270 nanometers – about 0.000001 inches. They carry a minute voltage.
Vibrations from bodily motions and sounds put part of the chip in very slight motion, making the voltage flux, thus creating readable electronic outputs. In human testing, the chip has recorded a variety of signals from the mechanical workings of the lungs and the heart with clarity, signals that often escape meaningful detection by current medical technology.
“Right now, medicine looks to EKGs (electrocardiograms) for information on the heart, but EKGs only measure electrical impulses. The heart is a mechanical system with muscles pumping and valves opening and shutting, and it sends out a signature of sounds and motions, which an EKG does not detect. EKGs also say nothing about lung function,” said Farrokh Ayazi, Ken Byers Professor in Georgia Tech’s School of Electrical and Computer Engineering.
Stethoscope-accelerometer combo
The chip, which acts as an advanced electronic stethoscope and accelerometer in one, is aptly called an accelerometer contact microphone. It detects vibrations that enter the chip from inside the body while keeping out distracting noise from outside the body's core like airborne sounds
“If it rubs on my skin or shirt, it doesn’t hear the friction, but the device is very sensitive to sounds coming at it from inside the body, so it picks up useful vibrations even through clothing,” Ayazi said.
The detection bandwidth is enormous - from broad, sweeping motions to inaudibly high-pitched tones. Thus, the sensor chip records all at once fine details of the heartbeat, waves the heart sends through the body, and respiration rates and lung sounds. It even tracks the wearer’s physical activities such as walking.
The signals are recorded in sync, potentially offering the big picture of a patient’s heart and lung health. For the study, the researchers successfully recorded a “gallop,” a faint third sound after the “lub-dub” of the heartbeat. Gallops are normally elusive clues of heart failure.
The researchers published their results in the journal npj Digital Medicine on February 12, 2020. The research was funded by the Georgia Research Alliance, the Defense Advanced Research Projects Agency (DARPA), the National Science Foundation, and the National Institutes of Health. Study coauthor Divya Gupta, M.D., a cardiologist at Emory University, collaborated in testing the chip on human participants.
Hermetically sealed vacuum
Medical research has tried to make better use of the body’s mechanical signals for decades but recording some – like waves traversing multiple tissues – has proven inconsistent, while others – like gallops – have relied upon clinician skills influenced by human error. The new chip produces high-resolution, quantified data that future research could match to pathologies in order to identify them.
“We are working already to collect significantly more data matched with pathologies. We envision algorithms in the future that may enable a broad array of clinical readings,” Ayazi said.
Though the chip’s main engineering principle is simple, making it work and then manufacturable took Ayazi’s lab ten years, mainly because of the Lilliputian scale of the gap between the silicon layers, i.e. electrodes. If the 2-millimeter by 2-millimeter sensor chip were expanded to the size of a football field, that air gap would be about an inch wide.
“That very thin gap separating the two electrodes cannot have any contact, not even by forces in the air in between the layers, so the whole sensor is hermetically sealed inside a vacuum cavity,” Ayazi said. “This makes for that ultralow signal noise and breadth of bandwidth that are unique.”
Detects through clothing
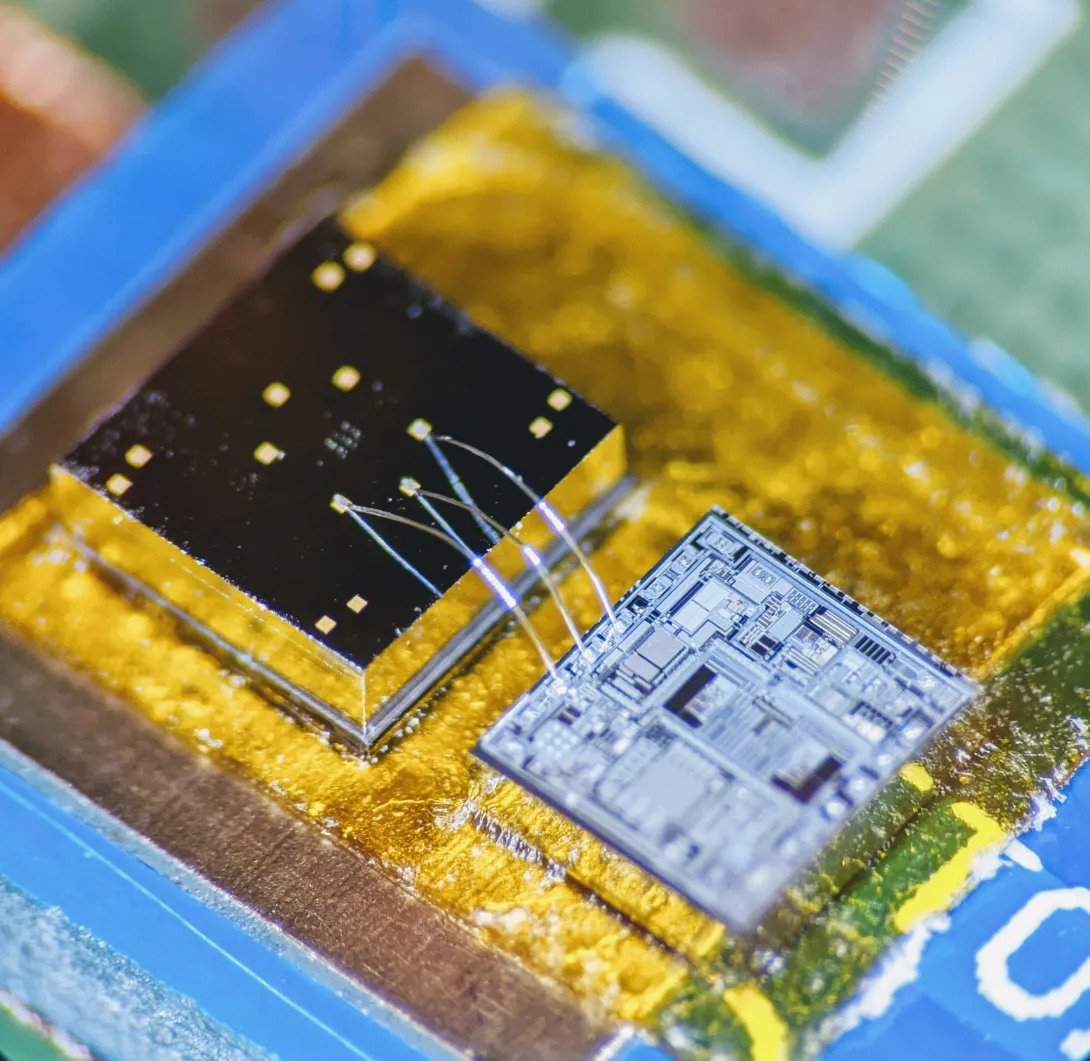
The researchers used a manufacturing process developed in Ayazi’s lab called the HARPSS+ platform (High Aspect Ratio Poly and Single Crystalline Silicon) for mass production, running off hand-sized sheets that were then cut into the tiny sensor chips. HARPSS+ is the first reported mass manufacturing process that achieves such consistently thin gaps, and it has enabled high-throughput manufacturing of many such advanced MEMS, or microelectromechanical systems.
The experimental device is currently battery-powered and uses a second chip called a signal-conditioning circuit to translate the sensor chip’s signals into patterned read-outs.
Three sensors or more could be inserted into a chest band that would triangulate health signals to locate their sources. Someday a device may pinpoint an emerging heart valve flaw by turbulence it produces in the bloodstream or identify a cancerous lesion by faint crackling sounds in a lung.
Here's how to subscribe to our free science and technology newsletter
Also read: Digital tool helps with tough COVID19 decision
These researchers co-authored the study: Pranav Gupta (first author), Mohammad Moghimi, Yaesuk Jeong and Omer Inan from Georgia Tech. The research was funded by the Georgia Research Alliance, the Defense Advanced Research Projects Agency (DARPA) Technology Office’s Advanced Inertial Micro Sensors program (contract # N66001-16-1-4064), and by the National Science Foundation/National Institutes of Health Smart and Connected Health Program (grant # R01 EB023808). The team’s work with human subjects was approved by Emory University and Georgia Institute of Technology Institutional Review Boards (IRB# H18248). Any findings, conclusions or recommendations are those of the authors and not necessarily of the sponsors.
Writer & Media Representative: Ben Brumfield (404-272-2780), email: ben.brumfield@comm.gatech.edu
Georgia Institute of Technology

What-if questions can torment a doctor making coronavirus retest decisions: What if a patient’s initial negative test was a false negative, and he or she needs a second test? What if they don’t need it, and a retest would use up a scarce test kit and treatments that other patients need?
Such challenges led Piedmont Healthcare in Atlanta to establish a paper-based decision tree for ordering COVID-19 retests, and researchers at the Georgia Institute of Technology turned it into an automated digital tool. Piedmont further developed the tool and has now built it into the hospital’s electronic medical record, where it influences the ordering of retests.
A user can answer their “ifs” by clicking through questions, and the “if-this-then-do-that” algorithm makes recommendations for best courses of action, ranging from immediately treating a patient for COVID-19 to retesting to consulting a specialist. The final decision remains with the physician.
The questions are deceptively simple, but the recommendations are not always obvious. That reflects the algorithm’s usefulness to fill gaps in thinking about the new sickness, which can confront clinicians with surprises.
“If a patient has not had close contact with positive patients and the first test came back negative, a physician may think the patient does not need to be retested. But actually, the patient may need a second test because they are in intensive care and also have suspicious chest X-rays,” said Georgia Tech graduate research assistant April Yu, who converted the decision tree into a digital tool.
“One of our big worries in using a brand-new test like the coronavirus test is that it will miss real cases, and this tool helps prevent that,” said Dr. Bronwen Garner, who helped develop the original decision tree and is an infectious disease specialist at Piedmont Healthcare. “It also helps reassure physicians when they get a negative result that it is probably a true negative.”
Suspenseful decision-making
A physician’s reaction to an initial negative test can mean life or death because the physician not only decides on follow-up testing but also on treatment pathways and quarantine.
“If you make a misstep in the thought process, it can lead to cascading impacts not only for the patient but also for healthcare professionals and family members, who may be exposed to the patient,” said Pinar Keskinocak, William W. George Chair and Professor in Georgia Tech’s Stewart School of Industrial and Systems Engineering. “This tool is meant to help doctors easily stay on the decision tree path.”
Michael O’Toole, executive director of Piedmont Healthcare’s quality improvement department, originally pictured doctors getting an automated version of the decision tree to use on their phones. O’Toole called Keskinocak, and she tapped Yu, a member of her research group.
“Literally within four hours they had it ready for us. It was incredible,” said O’Toole, a Georgia Tech alumnus who studied industrial and systems engineering.
“It was a very pleasant surprise,” said Dr. Garner, who is also a Georgia Tech graduate. “Automated tools are better than a paper format because they’re in the same format as orders in our electronic system. We get notifications in real time instead of having to remember to check a piece of paper.”
The tool is in place in the system where doctors order retests and is specific to Piedmont’s workflow. It may not be directly transferable to other health care systems.
Piedmont Healthcare simplified the logic even more, and the hospital built its own custom alerts to guide physicians on retesting. For cases that are more ambiguous, Piedmont Healthcare’s final version of the tool also gives physicians inside the hospital guidance to consult with their in-house infectious disease specialists.
If-this-then-retest
In her original version, Yu had turned the decision tree criteria into a short panel of questions with yes and no answers. It took her six iterations to arrive at her final version.
Yu’s version asked whether the patient:
- has a relevant ailment
- previously tested positive for coronavirus
- is now in an intensive care unit
- has worsening lung conditions
- shows telltale lung damage in imaging
- has been diagnosed with a different ailment
- the patient has had contact with someone else who tested positive for coronavirus.
On the back end, the algorithm guided the user through risks of coronavirus presence based on the answers.
“The steps were easy to follow, and the answers were color-coded for urgency with white, yellow, and red,” said Keskinocak, who also directs Georgia Tech’s Center for Health and Humanitarian Systems.
One bright yellow answer read: “This patient needs re-testing 24 hours after the initial test!” And there were further recommendations on how to handle the case.
Here's how to subscribe to our free science and technology newsletter
Also read: Advice on DIY masks
Writer & Media Representative: Ben Brumfield (404-272-2780), email: ben.brumfield@comm.gatech.edu
Georgia Institute of Technology
News Contact
Institute Communications

Georgia Tech Arts is still seeking projects for the 2021 ACCelerate: ACC Smithsonian
Creativity and Innovation Festival in Washington, DC. All Georgia Tech students, faculty, and staff are invited to apply by May 1, 2020.
Even if you do not have a finished project exploring the intersection of science,
engineering, art, design, and technology, we encourage you to speak with Es
Famojure at esther.famojure@arts.gatech.edu about your concepts.
Learn about Georgia Tech's 2019 participants for some inspiration.
The festival brings together all institutions included in the Atlantic Coast Conference to
celebrate creativity and innovation with a specific focus on science, engineering, arts, and
design. It will be held April 9 -11, 2021 at the Smithsonian National Museum of American
History.
Submit your project for consideration by May 1, 2020 to be considered.
News Contact
Es Famojure
esther.famojure@arts.gatech.edu
What-if questions can torment a doctor making coronavirus retest decisions: What if a patient’s initial negative test was a false negative, and he or she needs a second test? What if they don’t need it, and a retest would use up a scarce test kit and treatments that other patients need?
Such challenges led Piedmont Healthcare in Atlanta to establish a paper-based decision tree for ordering COVID-19 retests, and researchers at the Georgia Institute of Technology turned it into an automated digital tool. Piedmont further developed the tool and has now built it into the hospital’s electronic medical record, where it influences the ordering of retests.
A user can answer their “ifs” by clicking through questions, and the “if-this-then-do-that” algorithm makes recommendations for best courses of action, ranging from immediately treating a patient for COVID-19 to retesting to consulting a specialist. The final decision remains with the physician.
The questions are deceptively simple, but the recommendations are not always obvious. That reflects the algorithm’s usefulness to fill gaps in thinking about the new sickness, which can confront clinicians with surprises.
“If a patient has not had close contact with positive patients and the first test came back negative, a physician may think the patient does not need to be retested. But actually, the patient may need a second test because they are in intensive care and also have suspicious chest X-rays,” said Georgia Tech graduate research assistant April Yu, who converted the decision tree into a digital tool.
“One of our big worries in using a brand-new test like the coronavirus test is that it will miss real cases, and this tool helps prevent that,” said Dr. Bronwen Garner, who helped develop the original decision tree and is an infectious disease specialist at Piedmont Healthcare. “It also helps reassure physicians when they get a negative result that it is probably a true negative.”
Suspenseful decision-making
A physician’s reaction to an initial negative test can mean life or death because the physician not only decides on follow-up testing but also on treatment pathways and quarantine.
“If you make a misstep in the thought process, it can lead to cascading impacts not only for the patient but also for healthcare professionals and family members, who may be exposed to the patient,” said Pinar Keskinocak, William W. George Chair and Professor in Georgia Tech’s Stewart School of Industrial and Systems Engineering. “This tool is meant to help doctors easily stay on the decision tree path.”
Michael O’Toole, executive director of Piedmont Healthcare’s quality improvement department, originally pictured doctors getting an automated version of the decision tree to use on their phones. O’Toole called Keskinocak, and she tapped Yu, a member of her research group.
“Literally within four hours they had it ready for us. It was incredible,” said O’Toole, a Georgia Tech alumnus who studied industrial and systems engineering.
“It was a very pleasant surprise,” said Dr. Garner, who is also a Georgia Tech graduate. “Automated tools are better than a paper format because they’re in the same format as orders in our electronic system. We get notifications in real time instead of having to remember to check a piece of paper.”
The tool is in place in the system where doctors order retests and is specific to Piedmont’s workflow. It may not be directly transferable to other health care systems.
Piedmont Healthcare simplified the logic even more, and the hospital built its own custom alerts to guide physicians on retesting. For cases that are more ambiguous, Piedmont Healthcare’s final version of the tool also gives physicians inside the hospital guidance to consult with their in-house infectious disease specialists.
If-this-then-retest
In her original version, Yu had turned the decision tree criteria into a short panel of questions with yes and no answers. It took her six iterations to arrive at her final version.
Yu’s version asked whether the patient:
- has a relevant ailment
- previously tested positive for coronavirus
- is now in an intensive care unit
- has worsening lung conditions
- shows telltale lung damage in imaging
- has been diagnosed with a different ailment
- the patient has had contact with someone else who tested positive for coronavirus.
On the back end, the algorithm guided the user through risks of coronavirus presence based on the answers.
“The steps were easy to follow, and the answers were color-coded for urgency with white, yellow, and red,” said Keskinocak, who also directs Georgia Tech’s Center for Health and Humanitarian Systems.
One bright yellow answer read: “This patient needs re-testing 24 hours after the initial test!” And there were further recommendations on how to handle the case.
Here's how to subscribe to our free science and technology newsletter
Also read: Advice on DIY masks
Writer & Media Representative: Ben Brumfield (404-272-2780), email: ben.brumfield@comm.gatech.edu
Georgia Institute of Technology






COVID-19 has caught Pinar Keskinocak well prepared. For years, she has studied how societies manage pandemics, and how outbreaks overtax the health care system and wrack supply chains to worsen pandemics. Here she shares her insights.
Empty classrooms and supermarket shelves marked the beginning of the COVID-19 pandemic. But Keskinocak expects more signs of the times to come – such as pop-up pandemic clinics and the shortage and rationing of medical supplies beyond masks and ventilators.
Keskinocak is the director of the Center for Health and Humanitarian Systems at the Georgia Institute of Technology, which studies how government and private sectors can cooperate to handle health and humanitarian crises. And she is William W. George Chair and Professor in Georgia Tech’s H. Milton Stewart School of Industrial and Systems Engineering.
In previous research, Keskinocak’s team created a model that accurately ran the course of the 1918 Spanish flu pandemic, and when COVID-19 struck, her team was already in the middle of modeling how special clinics could significantly slow a pandemic. In the meantime, temporary clinics in Wuhan, China, appear to have validated her model.
Healthcare expansion now
The surge of COVID-19 patients pushed Italy’s health care system into a very ugly crisis, and the U.S. needs to take measures now to handle similar patient surges. Pandemics often strike in two waves or more, and the second is usually the worst, so measures need to be lasting, Keskinocak said.
Even without COVID-19, the U.S. healthcare system has been under strain. Emergency rooms are often overcrowded; it takes a long time to schedule an appointment, and there is a chronic shortage of nursing staff.
[Read Keskinocak's guest op-ed in the New York Daily News: COVID clinics now]
“We need to expand capacity and unleash creative flexibility in our healthcare systems. We should use more telemedicine and create self-service stations for testing. I would particularly like to see specialized COVID-19 clinics established now,” Keskinocak said.
“Special clinics could be separate spaces in existing facilities or standalone facilities. As COVID-19 spreads, we expect a lot more people with cold- and flu-like symptoms to seek testing and care. The healthcare capacities are just not there for a business as usual approach, and taking it could harm patients by delaying care and increasing risk of infection.”
Gathering COVID-19 patients in tight spaces like waiting rooms with other patients would increase the coronavirus’ spread, and patients with preexisting conditions could face mortal threat. Contagion could also spread into hospitals.
“Dedicated pandemic clinics could implement targeted hygiene, air filtration, and specialized protective equipment beyond masks and gloves for healthcare workers. They can tailor workflows to test and care for patients quickly and effectively and keep them away from other patients and staff,” Keskinocak said.
Payment needs to be easy, too, including financing the uninsured. In the middle of a public health emergency, it is vital to not get bogged down by restrictions meant for normal times.
Potentially dangerous shortages
Toilet paper will make a comeback in supermarkets, but in its place, life-saving medications could become perilously scarce. Countries need to act now to prevent this from compounding the COVID-19 crisis.
“Dwindling availability of hospital beds, ventilators, and personal protective equipment like masks and gloves during a patient surge – those are the obvious things. But we could also see shortages of items like asthma medication or antidepressants. Worst case, even food supplies could run low,” Keskinocak said.
[Read Keskinocak's guest op-ed in The Hill: medical supply chain dangers]
Here’s how shortages work and can lead to price gouging and also rationing. The latter can have good effects.
“Shortages are the result of supply-demand imbalance caused by either an unexpected increase in demand or unexpected decrease in supply or both. Shortages are common in crises such as natural disasters or health emergencies. But given the worldwide slowdown of economic activity in pandemics, disruptions could get much worse this time,” Keskinocak said.
“Supply chains are actually intricate webs of multiple parts that span the globe. Pandemics damage many of those parts, and it can take time to recover. This creates a more serious and worrisome imbalance between supply and demand.”
Toilet paper will return because people fear-hoard it in a panic but consume it at normal rates. When the panic runs its course, demand slows back down to the actual rate of consumption and its normal supply chain, which is relatively simple, catches up.
“With medicine and healthcare services and supplies, the increase in demand is typically already in line with consumption, so a shortage in supply or increase in demand can create a supply-demand gap that continues for a long time,” Keskinocak said. “Medical supply chains are also very complex and fragile.”
Future vaccine distribution
In normal times, most supply chains work at a plodding pace, and when crisis strikes, it is tough to ramp them up due to expensive equipment, complex logistics, and strict regulations, particularly in health care. Even temporary shortages of medicines and medical devices can have consequences for patients who need them.
“If shortages become serious, rationing – with a priority allocation to those most in need – can help balance demand and supply for critical items like medications.”
Once created and approved, the production of vaccines or antivirals for COVID-19 will ramp up slowly and could be in short supply at first. Decision-makers need plan investments now in the supply chains necessary for their effective distribution.
This will include painful, necessary decisions like prioritizing first doses for healthcare workers, people with pre-existing conditions, and the elderly. The current system of restocking vaccines in the U.S. after initial distribution also has serious gaps that need fixing to save many more lives.
In the meantime, social distancing is one of the best ways to protect everyone and reduce the patient surge into clinics. Do it if you or anyone in your household has any cold-like symptoms.
[Read Keskinocak's commentary on social distancing on AJC.com]
Also read: Vaccine Supply Gaps Can Make Pandemics Deadlier
Media contacts: Ben Brumfield (ben.brumfield@comm.gatech.edu) and John Toon (john.toon@comm.gatech.edu)